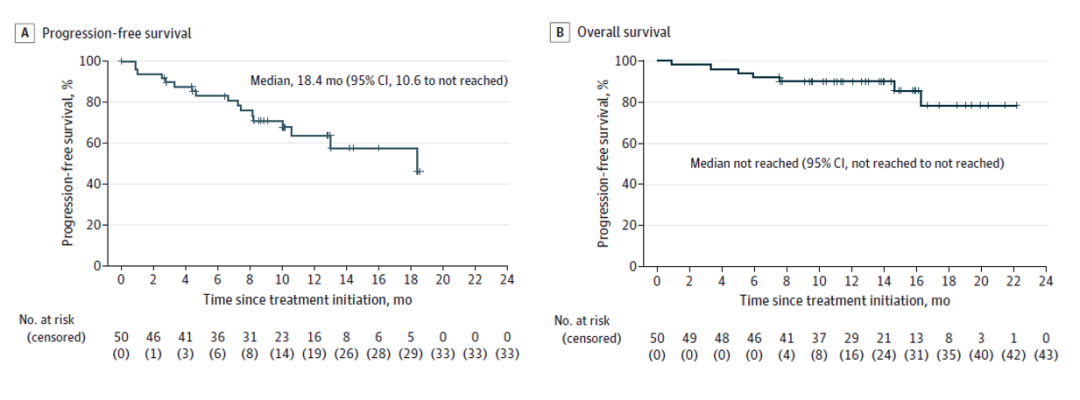
北京时间2023年6月2日,由北京大学肿瘤医院黑色素瘤与肉瘤科郭军教授与斯璐教授团队开展的卡瑞利珠单抗联合Apatinib/ target=_blank class=infotextkey>阿帕替尼与替莫唑胺一线治疗晚期肢端黑色素瘤临床试验(CAP-03研究)全文发表于医学权威期刊美国医学会杂志肿瘤子刊《JAMA Oncology》(IF:33.006)[1],结果显示,卡瑞利珠单抗联合Apatinib/ target=_blank class=infotextkey>阿帕替尼与替莫唑胺一线治疗晚期肢端黑色素瘤,客观缓解率(ORR)为64.0%,疾病控制率(DCR)达到88.0%,中位无进展生存期(PFS)为18.4个月,整体安全性可控。卡瑞利珠单抗联合阿帕替尼与替莫唑胺的“三药”组合方案为晚期肢端黑色素瘤患者带来新的治疗选择。 CAP-03研究在线发表于JAMA Oncology 肢端黑色素瘤是指位于手掌、足底和甲下的黑色素瘤,其发病率约占亚洲人群黑色素瘤的40%[2,3]。与皮肤黑色素瘤相比,肢端黑色素瘤肿瘤突变负荷较低,更具有侵袭性[4-6]。免疫治疗作为晚期皮肤黑色素瘤的标准一线治疗[7],在晚期肢端黑色素瘤中疗效并不令人满意[8-12],需要探索针对晚期肢端黑色素瘤更有效的一线治疗方法。 抗血管生成药物与免疫检查点抑制剂(ICIs)联用可诱导肿瘤血管正常化,缓解缺氧,调节肿瘤免疫微环境,促进抗肿瘤免疫[13,14]。阿帕替尼是一种靶向血管内皮生长因子受体(VEGFR)2的小分子酪氨酸激酶抑制剂,可以抑制黑色素瘤的血管生成[15,16]。一项探索性研究显示,阿帕替尼在既往接受过治疗的转移性黑色素瘤患者中的客观缓解率(ORR)为13%,中位无进展生存期(PFS)为4.0个月[17]。在一项Ⅱ期研究中,卡瑞利珠单抗联合阿帕替尼一线治疗晚期肢端恶黑患者,ORR为24%,中位PFS为7.4个月[18]。尽管这种组合拥有良好的临床价值,但更有效的方案依然值得被探索。 替莫唑胺是一种经典的细胞毒性药物,与达卡巴嗪疗效相当,在晚期黑色素瘤患者的Ⅲ期试验中,ORR为13%,中位PFS为1.9-2.4个月[19,20]。替莫唑胺可以通过消耗调节性T细胞,增强细胞毒性T淋巴细胞(CD8+T细胞)对肿瘤相关抗原的反应,促进T细胞浸润到黑色素瘤增强免疫治疗的效果[21,22]。本研究旨在探索卡瑞利珠单抗联合阿帕替尼与替莫唑胺一线治疗晚期肢端恶黑患者的疗效与安全性。 CAP-03研究亮相国际顶级学术期刊全球首创三联方案取得优异成果 CAP-03研究是一项研究者发起的Ⅱ期单臂临床试验,主要入排标准为:年龄在18-75岁;组织学证实无法切除的Ⅲ期或Ⅳ期肢端恶性黑色素瘤;晚期未接受过系统性抗肿瘤治疗;BRAF V600E野生型;Eastern Cooperative Oncology Group (ECOG) 评分0或1分;预期生存期至少为3个月;根据实体瘤应答评价标准(RECIST)1.1版至少有一个可测量的病变,患者接受静脉注射卡瑞利珠单抗200mg,每2周1次,口服阿帕替尼250mg,每天1次,每4周的前1-5天静脉注射替莫唑胺200mg/m2。治疗直至疾病进展、不可耐受的毒性、撤回知情同意或完成2年治疗。 研究主要终点为客观缓解率(ORR),次要终点包括无进展生存期(PFS)、至反应时间(TTR)、反应持续时间(DOR)、疾病控制率(DCR)、总生存(OS)和安全性。 图1.研究设计 共50例患者纳入并接受治疗。中位随访时间为13.4个月(IQR,9.6-16.2)。ORR为64.0%(32/50;95%CI,49.2%-77.1%)。中位TTR和DOR分别为2.7个月(IQR,0.9-2.9)和17.5个月(95%CI,12.0-未达到)。DCR为88.0%(44/50;95%CI,75.7%-95.5%)。 图2.瀑布图与泳道图 中位PFS为18.4个月(95%CI,10.6-未达到)。 图3.PFS(左)与OS(右)的K-M曲线 卡瑞利珠单抗联合阿帕替尼和注射用替莫唑胺的三药联合方案在全球属于首创,其在一线治疗晚期肢端黑色素瘤的研究取得了令人振奋的结果。考虑到既往研究中PD-1单药或联合CTLA-4治疗晚期肢端黑色素瘤ORR在16%-45%,中位PFS在3.0-6.6个月[8-11],本研究所取得的疗效结果令人振奋,且安全性良好可耐受。本研究的出色数据提供了肢端黑色素瘤一线治疗的新模式,满足了目前对于肢端黑色素瘤治疗方案的迫切需求。值得一提的是,该三药联用是真正惠及我国肢端黑色素瘤患者的创新方案。 总结与展望 CAP-03研究凭借其创新性和令人惊喜的疗效,成功入选2022 ASCO口头报告环节并于今年在顶级学术期刊《JAMA Oncology》全文发表,卡瑞利珠单抗联合阿帕替尼和替莫唑胺的三联方案也成功纳入2023版《CSCO黑色素瘤诊疗指南》,获一线治疗晚期肢端恶性黑色素瘤Ⅱ级推荐。 图4.卡瑞利珠单抗联合阿帕替尼和替莫唑胺方案获 CSCO指南推荐 目前郭军教授团队正在同步开展基于卡瑞利珠单抗联合治疗的随机对照Ⅲ期临床研究。期待后续的研究继续取得积极结果,进一步提高以卡瑞利珠单抗为基础的三联方案在CSCO指南乃至国际指南对肢端黑色素瘤一线治疗的推荐级别,成为晚期肢端黑色素瘤一线治疗新的选择(内容来源:爱医时空)。 参考文献: 1. Guo J, Si L,et al. Camrelizumab Plus Apatinib and Temozolomide as First-Line Treatment in Patients With Advanced Acral Melanoma: The CAP 03 Phase 2 Nonrandomized Clinical Trial. JAMA Oncol. 2023 Jun 1. doi: 10.1001/jamaoncol.2023.1363. Epub ahead of print. PMID: 37261804. 2.Chi Z, Li S, Sheng X, et al. Clinical presentation, histology, and prognoses of malignant melanoma in ethnic Chinese: a study of 522 consecutive cases. BMC Cancer. 2011;11:85. doi:10.1186/1471-2407-11-85 3.Fujisawa Y, Yoshikawa S, Minagawa A, et al. Clinical and histopathological characteristics and survival analysis of 4594 Japanese patients with melanoma. Cancer Med. 2019;8(5):2146-2156. doi:10.1002/cam4.2110 4.Curtin JA, Fridlyand J, Kageshita T, et al. Distinct sets of genetic alterations in melanoma. N Engl J Med. 2005;353(20):2135-2147. doi:10.1056/NEJMoa050092 5.Hayward NK, Wilmott JS, Waddell N, et al. Whole-genome landscapes of major melanoma subtypes. Nature. 2017;545(7653):175-180. doi:10.1038/nature22071 6.Newell F, Johansson PA, Wilmott JS, et al. Comparative Genomics Provides Etiologic and Biological Insight into Melanoma Subtypes. Cancer Discov. 2022;12(12):2856-2879. doi:10.1158/2159-8290.CD-22-0603 7.National Comprehensive Cancer Network. (NCCN) Clinical Practice Guidelines in Oncology. Melanoma: Cutaneous, Version 3. 2022. https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf Accessed April 11, 2022. 8.Nakamura Y, Namikawa K, Yoshino K, et al. Anti-PD1/ target=_blank class=infotextkey>PD1 checkpoint inhibitor therapy in acral melanoma: a multicenter study of 193 Japanese patients. Ann Oncol. 2020;31(9):1198-1206. doi:10.1016/j.annonc.2020.05.031 9.van Not OJ, de Meza MM, van den Eertwegh AJM, et al. Response to immune checkpoint inhibitors in acral melanoma: A nationwide cohort study. Eur J Cancer. 2022;167:70-80. doi:10.1016/j.ejca.2022.02.026 10.Bhave P, Ahmed T, Lo SN, et al. Efficacy of anti-PD-1 and Ipilimumab alone or in combination in acral melanoma. J Immunother Cancer. 2022;10(7):e004668. doi:10.1136/jitc-2022-004668 11.Nakamura Y, Namikawa K, Kiniwa Y, et al. Efficacy comparison between anti-PD-1 antibody monotherapy and anti-PD-1 plus anti-CTLA-4 combination therapy as first-line immunotherapy for advanced acral melanoma: A RETrospective, multicenter study of 254 Japanese patients. Eur J Cancer. 2022;176:78-87. doi:10.1016/j.ejca.2022.08.030 12.Tawbi HA, Schadendorf D, Lipson EJ, et al. Relatlimab and nivolumab versus nivolumab in Untreated Advanced Melanoma. N Engl J Med. 2022;386(1):24-34. doi:10.1056/NEJMoa2109970 13.Ramjiawan RR, Griffioen AW, Duda DG. Anti-angiogenesis for cancer revisited: Is there a role for combinations with immunotherapy? Angiogenesis. 2017;20(2):185-204. doi:10.1007/s10456-017-9552-y 14.Yi M, Jiao D, Qin S, Chu Q, Wu K, Li A. Synergistic effect of immune checkpoint blockade and anti-angiogenesis in cancer treatment. Mol Cancer. 2019;18(1):60. doi:10.1186/s12943-019-0974-6 15.Liu Z-J-L, Zhou Y-J, Ding R-L, et al. In vitro and in vivo apatinib inhibits vasculogenic mimicry in melanoma MUM-2B cells. PLoS One. 2018;13(7):e0200845. doi:10.1371/journal.pone.0200845 16.Zhang J, Liu P, Zhang Z, et al. Apatinib-loaded nanoparticles inhibit tumor growth and angiogenesis in a model of melanoma. Biochem Biophys Res Commun. 2020;521(2):296-302. doi:10.1016/j.bbrc.2019.10.084 17.Yuan S, Fu Q, Zhao L, et al. Efficacy and Safety of Apatinib in Patients with Recurrent or Refractory Melanoma. Oncologist. 2022;27(6):e463-e470. doi:10.1093/oncolo/oyab068 18.Wang X, Wu X, Yang Y, et al. Apatinib combined with Camrelizumab in advanced acral melanoma patients: An open-label, single-arm phase 2 trial. Eur J Cancer. 2023;182:57-65. doi:10.1016/j.ejca.2022.12.027 19.Middleton MR, Grob JJ, Aaronson N, et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol. 2000;18(1):158-166. doi:10.1200/JCO.2000.18.1.158 20.Kaufmann R, Spieth K, Leiter U, et al. Temozolomide in combination with interferon-alfa versus temozolomide alone in patients with advanced metastatic melanoma: a randomized, phase III, multicenter study from the Dermatologic Cooperative Oncology Group. J Clin Oncol. 2005;23(35):9001-9007. doi:10.1200/JCO.2005.01.1551 21.Iversen TZ, Brimnes MK, Nikolajsen K, et al. Depletion of T lymphocytes is correlated with response to temozolomide in melanoma patients. Oncoimmunology. 2013;2(2):e23288. doi:10.4161/onci.23288 22.Tan KW, Evrard M, Tham M, et al. Tumor stroma and chemokines control T-cell migration into melanoma following Temozolomide treatment. Oncoimmunology. 2015;4(2):e978709. doi:10.4161/2162402X.2014.978709 
“双艾”组合再接再厉探索晚期肢端黑色素瘤创新方案



更多